
Fractures, fractures and more fractures
Basics of fractures for juniors & medical students!

Fracture basics for a medical student / junior doctor
I had my orthopaedic rotation around 3 months ago and I learnt quite a lot, so I’m just going to list what I got taught down here and pass them on to you. A gift, from me to you.
I was taught these by an orthopaedic surgery resident.
A fracture in simple terms is the cracking or breaking of a bone. To describe what a fracture is in an x-ray; it is the discontinuation of bone.
So, when looking at an x-ray for a fracture, pick a starting point on the bone and just go around following the white line of the bone. If there is any breaking of the line or discontinuation = possible fracture
Here, try it out: Trace the white lines on this image from one point and go all the way around. Can you spot the fracture?

Case courtesy of Dr Servet Kahveci, <a href="https://radiopaedia.org/?lang=us">Radiopaedia.org</a>. From the case <a href="https://radiopaedia.org/cases/85771?lang=us">rID: 85771</a> 
Case courtesy of Dr Piotr Gołofit, <a href="https://radiopaedia.org/?lang=us">Radiopaedia.org</a>. From the case <a href="https://radiopaedia.org/cases/48267?lang=us">rID: 48267</a> Remember that the more dense an organ/item, the whiter it will appear on an x-ray. That is why, when you look at a bone in an x-ray, the middle part is less white than the sides, because the side is the compact bone which is denser than the middle spongy part of the bone.

Remember, bones are 3D. When looking at an x-ray you are looking at a 2D image. Looking at it straight on (x-ray image) there’s more bone on the sides due to the curvature for the x-ray beam to reflect off of.
One x-ray image = not the full story. TWO views are needed to cover two planes. When you get an AP (Anteroposterior) x-ray, you are only going to see what’s wrong with the sides of the bones i.e 3pm and 9pm from the patient perspective. What if the fracture is in the 12pm position? or 6pm? an AP view won’t show you that. You’ll need a lateral view of the bone too. Here is a perfect example.

Top image: You can see that there is a fracture on the bone on the right side. Clear and obvious fracture. You could diagnose it and move on. However, if you asked for a second image angle (bottom one: lateral), you would see that there is also a fracture on the other side of the bone. This could lead to either the same diagnosis and same treatment, or different diagnoses and different treatment. It is always better to catch something and note it down rather than missing it.
Here is another example. The below image is the frontal imaging and you can barely see the fracture, but it is there, this one image doesn’t give you much information, now look at the lateral image and see what it can show you.

Anterior image 
Lateral image When someone comes in with a fracture of a part of their body, always remember to get imaging for the joints above and below / adjacent joints. So, if someone comes in with really bad shin pain after being tackled in football, and you highly suspect a tibia/fibula fracture, you should also ask for an x-ray of the ankle and knee. The aim is to the the above and below joints and to also see the bones between.
If someone messes up their elbow, get a scan of their wrist and shoulder.
If you suspect a femur fracture, image the knee and hip. Humerus? Elbow and Shoulder. You get the point.
There are open and closed fractures. The open and closed is referring to the skin. If the skin is intact then it is a CLOSED fracture. Has the bone penetrated the skin and opened it up? then it’s an OPEN fracture. Which one is worse? you guessed it. OPEN. Because open fractures can lead to infections and take longer to heal.
Someone brought in with a fracture? You are the FY1/FY2 in A&E? Don’t panic. Follow these steps.
A to E assessment to stabilise the patient
The wound needs urgent cleaning if its an open fracture - book the OR & escalate
Antibiotics if open fracture
Painkillers for obvious reasons
Imaging. Remember points 3 and 4!!! Get multiple angles and above and below the ‘Main’ area.
Refer to ortho team for urgent fixation / surgery / further planning / Escalation.
Think about the plastics team if necessary
Take a deep breath and sip on your tea and relax (or just sip on your water very quickly and run off to your next patient) (oh, obviously don’t forget to document obviously lol)
There is external fixation and internal fixation. Fixation is literally what you think. It is FIXATING a bone. This can be either a temporary solution or permanent.
Internal fixation: When you fixate the bone internally. It is usually a permanent solution and patients can continue to live with the fixator inside them until they are fully healed and in some select cases, do not even need to be removed. Here are some examples of internal fixators
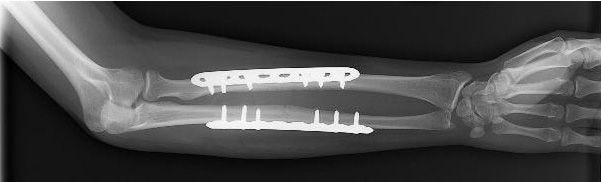
n this x-ray, broken bones in a forearm are held in position with plates and screws while they heal. 
A broken bone in this patient’s ankle is held in position with plates and screws. 
This x-ray shows a healed shinbone fracture treated with intramedullary nailing. External fixation: When you fixate the bone externally. Usually external fixation is a temporary solution. They are easy anf fast to apply and are put on when a patient has multiple injuries and not ready for a longer more permanent surgery. The external fixator can stay in place until the patient is ready for the main surgery. Other times, the external fixator can be used as a permanent solution. Here are some examples:

This patient’s fractured thighbone has been stabilized with external fixation. The fixator will be removed when surgery to repair the fracture can be performed safely.
THINK SYSTEMATICALLY. If someone falls from a building and lands on their feet. Think about what could be damaged. Start from point of impact and work up/down. So start from the feet, the ankles, tibia, fibula, knee, femur or hips. The Spine as well. IF someone was in a high-speed collision in a car. Think about what it could be. Knees, hips, tibia, fibula, chest, wrists, elbows, shoulders. Just to add another example. If someone is running and falls on their hands and assuming they ONLY fell on their hands. You check the hands, wrist, radius, ulna, elbow, humerus, elbow. Make sense?
If they fell and the whole body made contact with the floor, then obviously you need to check the head, ribs, hips, legs, feet etc.
Don’t forget dislocations! Okay, they have a radius bone fracture and no other fracture anywhere else, cool. But have you ruled out a dislocation of the joints too?
The way to do it is to start thinking of the body part that was hit by the impact first and work your way up / down.
Fractures are the main topic. Don’t forget dislocations too. A fracture + a dislocation is a completely different diagnosis. Some examples of the combination:
Galeazzi fracture - Radial shaft fracture with associated dislocation of the distal radioulnar joint
Barton's fracture - Distal radius fracture (Colles'/Smith's) with associated radiocarpal dislocation










I hope you find this guide helpful and I hope you learnt something!
Images of the fixations are courtesy of: https://orthoinfo.aaos.org/en/treatment/internal-fixation-for-fractures/